
"Adapted from my second book, Breastfeeding Works! Simplifying breastfeeding in the 21st century"
Far too many breastfeeding women come to grief unnecessarily with mastitis. Most of the problems relate to unhelpful community folklore about mastitis prevention and management. Unfortunately, this includes much of the advice given by health professionals who have generally also not been exposed to better information.
Overflowing with milk
By contrast with the almost universal preoccupation Westerners have with undersupply, rampant oversupply is quite common for most new mothers in the early postnatal weeks. If mothers need (or wish) to express milk, this is the easy time to do it! The greatest downside to these wonderfully novel ‘Mae West breasts’ is that many people believe such large and obviously overfull equipment is a necessity for successful breastfeeding! (122)
Such beliefs create unnecessary anxiety for women who do not experience the same overenthusiastic start to their breastfeeding career, yet have a perfectly adequate milk supply in the early weeks. Women need reassurance that this is just as normal as the ‘Mae West’ experience – and even more likely for second, third and other lactations. The ‘biochemical factories’ (breasts) are more efficient by then at getting subsequent lactations going!


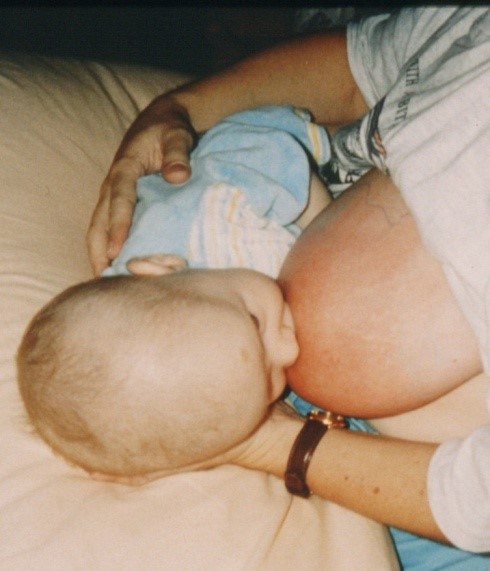
This mother’s right breast is overfull and hard (above left). She is right-handed and has been having trouble attaching her baby to the right side with her left hand and arm. As a result, her right breast was not as well drained after feeds as the left. Vibration used on this breast for ten minutes (above right) gave her welcome pain relief as well as softening the breast enough so her six day old baby could attach well and feed. A lumpy area in the breast also felt better from the vibration, and improved further after this feed. Supporting her left wrist with her right hand and learning to use her legs for arm support solved her attachment problem. In this case, she had been unnecessarily using her spare right hand to hold the breast for attachment. More vibration applied hourly for ten minutes over the next few hours – along with a few more breastfeeds – completely resolved her problems.
It is the mother’s job to keep her breasts comfortable to live with, especially in the early ‘over the top’ phase of her lactation when she may experience some engorgement. Because of low supply paranoia, new mothers with breastfeeding problems are frequently put on Domperidone (Motilium) in the early weeks, but then suffer from blocked ducts, mastitis and breast infections from unpleasantly enhanced milk production. It is more appropriate to resolve breastfeeding problems as quickly as possible. If negative conclusions are being drawn from low volumes of expressed milk, the answer may lie in improving the mother’s expressing technique and to review whether or not her pump suits her breasts. Pumps are not ‘one size fits all’!

Other than keeping her breasts well drained with a well attached baby (which means no pain is involved!!), she should be encouraged to use a vigorous level of vibration for sore or ‘lumpy’ breasts. Vibration eases pain, softens breasts and breaks up any ‘lumps and bumps’. At least ten minutes per hour of vibration (without heat!) applied through clothing to sore breasts is an easy, effective and non-invasive way to relieve breast discomfort and to resolve blocked ducts very quickly! (pictured right) Although breast massage is usually recommended, I don’t find it accomplishes much – vibration on sore breasts is far more effective!
Mothers love vibration on sore, overfull breasts! Even within a few minutes, the breast can be softened enough for a baby to attach and feed
Engorgement sometimes happens at inconvenient times and places, when mothers do not necessarily have a massager/vibrator unit to use just when they need it. Because ‘necessity is the Mother of Invention’, desperation sometimes causes wonderful flashes of inspiration. Consequently, women have thought about what else is available that vibrates! They have used items such as:
- an electric toothbrush
- sex ‘toys’
- electric shaver (with the cover left on)
- kitchen mixer-beater unit (minus the beaters!)
- an orbital sander or other power tools
Obviously, if using items that are not purpose built as massager units, mothers must take great care to ensure none of the moving parts are anywhere near them!!
Heat is often recommended for sore, overfull breasts. Unfortunately, it is misguided advice and can be expected to worsen problems because symptoms are the result of inflammatory feedback processes in overfull breasts. You would not be advised to put heat on any other inflamed part of your body!!
As breasts become overfull, inflammatory feedback mechanisms come into effect, reducing milk secretion rates and alerting a mother to the need to breastfeed.
‘Mastitis’ is a general term, meaning ‘inflamed breast’. Breasts are very resilient in their response to mastitis. Breast infections do not generally follow on from mastitis as long as mothers know what to do about it and act promptly!
Applying heat to such breasts is CONTRAINDICATED because they are already inflamed!
Before the milk ‘comes in’, babies have the advantage of learning to feed from soft breasts. If they feed with good attachment so their mothers do not suffer any nipple damage, there is usually a smooth transition for both mother and baby as the milk comes in. This is because an effective, well attached baby who feeds often enough will prevent breasts from becoming unpleasantly overfull and hard, greatly reducing the potential for engorgement. A few ounces of prevention are more sensible than ten pounds of cure.
In the early postnatal weeks, at least one night breastfeed is generally an important priority to prevent early morning engorgement. It is not pleasant to wake up with two matching Rocks of Gibraltar on your chest!

This mother needed to express forty ml of milk from her overfull breast (above) before it felt comfortable and was soft enough for her baby to attach and feed. The redness was gone by the time her baby came off the breast.
If breasts become too hard, babies struggle to attach well and to ‘milk’ hard breasts with the muscular actions needed. Newborns often just mouth around the nipple, or attach briefly and ‘fall off’ without really attempting to feed. If they manage to attach, their feeding efforts often cause damaged nipples and painful feeds for their mothers. Forestalling trouble involves softening hard breasts before feeds by expressing off some milk and/or using vibration on them. When mothers need to express milk to soften breasts for feeding or comfort, they may hear opinions that it should be restricted to very small volumes of milk (such as five to ten ml). The rationale is that, ‘You’ll make things worse because expressing larger volumes will make even more milk!’ Not so! If you are uncomfortable with engorgement, you’ve already made the milk that is causing you problems!
If bras are not large enough to be comfortable when a mother is overfull, she may do better without one. Clothing that is too tight can further interfere with the breasts’ lymphatic drainage. A large front-opening shirt worn as usual but tied comfortably between heavy breasts to provide support is more likely to please mothers in this situation than a bra that is too small.
Possible consequences of unrelieved hard breasts:
- engorgement
- painful breasts
- constant leaking (although it is not always linked to overfullness)
- blocked ducts
- galactocoeles (milk retention cysts)
- mastitis
- breast infections
- attachment difficulties
- nipple damage
- reduced milk flow from overfull breasts
- breast refusal
- formula supplementation of the baby
- weaning
In the hormone-enhanced days of early motherhood, some mothers make huge amounts of milk and NEED to express off some of the excess for comfort AND to prevent other problems. Unfortunately, I have seen too many women who were warned off the large milk volumes they should’ve expressed, who could’ve later written their own books on breast problems! Certainly, if mothers express, say between fifty and a hundred ml before each feed for at least a few days, they might find they’ve been ‘blessed with a few buckets more’, but this is not normally what mothers need for relief. In fact, ONE complete expressing session, where as much as possible is expressed from both breasts, is sometimes a very good idea, a bit like ‘starting again with a clean slate’.
Otherwise, total volumes expressed for comfort are generally:
- only a few times a day
- for only a few days until the breasts’ over-enthusiasm abates
- between ten and fifty ml, but sometimes may need to be considerably more if breasts are really ‘backed up’ with milk
If there is a persisting problem with rampant oversupply, other measures can be taken (discussed later in this chapter):
- cabbage leaves
- one dose of sage tea
One mother pumped off 200ml in 20 minutes, before she and I were both happy about her breast comfort! She didn’t need to do any more expressing after this because her week old baby could breastfeed well from that point. At this early stage of lactation, large milk volumes can be made regardless of what the baby’s actual needs are. This is very handy if you have birthed twins, triplets or quads, but can be a bit overwhelming if you have only one baby!
Other possible contributing factors to persisting oversupply:
- some maternal drugs
- some herbal treatments used by the mother
- mothers’ unique endocrine functions, possibly including underlying conditions such as underactive thyroid or pituitary tumour
- infant feeding effectiveness may not be up to keeping breasts well enough drained. In this case, weight gains may not be good, and the baby’s nappy output obviously not very adequate
- a baby’s feeding pattern may be fine for the baby but too infrequent for his mother’s needs
- occasionally, babies who are frequently on the breast overstimulate milk secretion, especially if they just suck and nuzzle rather than drink
- sometimes babies with large weight gains are being put to the breast more often than strictly needed, and the extra breast stimulation keeps milk production at an uncomfortable level. Mothers may need to give these babies a dummy to satisfy their suck needs. This is not common, and probably relates to these women’s individual endocrine responses. In other words, hormones!!
- excessive fluid intake by the mother? It is very unusual for this to cause oversupply, but I have had a few cases in twenty years. Usually, excessive fluid intake just means more urine output rather than more milk
Management of short-term acute oversupply, mastitis and breast infections
- the primary focus needs to be on good breast drainage, along with reducing the inflammatory response causing the symptoms. The baby’s attachment should not cause pain or nipple damage
- the baby should not be offered any breast substitutes, and should put to the breast as often as he is interested. If this is not possible, the milk needs to be expressed and fed to the baby in preference to using artificial baby milks. An effectively feeding baby will generally do a far better job of draining breasts than any breast pump – and far more pleasantly (140)
- the mother may need to express milk for breast comfort if the baby is not doing enough to help the mother out! ‘Expressing for comfort’ may mean taking off between ten and fifty ml of excess milk. However, ONE ‘complete’ expression of the breasts may resolve an acute problem entirely because it relieves pressure on lymph return and milk production feedback mechanisms. Note that ‘complete’ means ‘as much as a mother can express off at one time’ – there’s no such thing as an ‘empty’ breast!
- anti-inflammatory drugs such as ibuprofen (Nurofen) or Voltarin should be taken three times daily after meals to relieve symptoms of acute oversupply, particularly the inflammatory response. Although aspirin is anti-inflammatory, it is not nearly so much so as Nurofen, Voltarin or other nonsteroidal anti-inflammatories. Paracetamol can be taken as well if extra pain relief is needed
- although pleasant massage for any ‘lumpy’ or engorged areas has been traditionally recommended, I don’t find it achieves much, other than it is comforting. Any massage should be done only by the mother – overfull breasts are easily bruised in the first two weeks after birth, resulting in further problems with pain and drainage
- in place of massage, I can strongly recommend the use of an electric massager-vibrator unit – but without the heat setting! I find this to be the quickest, most effective and pleasant way for the mother to resolve breast problems. It is ideal for her to feed the baby (or express) from the affected breast/s soon afterwards
- vibration helps resolve ‘lumps’ and blocked ducts and is very comforting. It can also be used as often and for as long as the mother wishes, since it does not cause tissue damage. At least ten minutes per hour on ‘lumpy’ breasts or threatening mastitis is a good battle plan for resolving trouble! The mother should persist with this until her symptoms disappear
a Reverse Pressure technique
can be used to soften the areolas of engorged breasts. The mother uses her thumb and fingertips to press inwards around the base of her nipple and then to press them in towards each other under the nipple. The pressure should be maintained for some seconds, using constant firm pressure, then the fingers removed before repeating it on another part of her areola until it has softened enough to let the baby attach well and feed. If the areola tissue is very hard, the pressure may initially need to be less, but increased steadily as the tissue permits it. She should do this firmly but gently enough to avoid any more pain than she is already in and certainly without causing bruising. Nobody other than the mother should do this to her breasts because it is too easy for others to bruise them with more pressure than is safe. She is attached to her nerve endings, which give pretty good warning of anything potentially damaging! If no source of vibration is available, this technique may be the next best option
- warmth on breasts before expressing or feeding may assist the milk ejection reflex if it is inhibited by pain BUT I am not enthusiastic about warmth on oversupplied breasts because they are already overheated by the breasts’ feedback mechanisms! There is far too much advice still wrongly given about putting heat on sore breasts! Too many people over-interpret such advice, thinking that if a little is good, then a lot more must be that much better!! Heat applied to breasts helps increase milk production! (145)
- if breastfeeding or expressing isn’t enough to relieve oversupply, cold cabbage leaves applied two hourly to breasts (for up to a total of six hours) after feeding or expressing helps to reduce inflammation and blood flow in the breasts, easing engorgement and decreasing oversupply. Longer than six hours may overly reduce milk production. Cold cabbage leaves seem more effective and preferable to mothers than just cold compresses. Cabbage leaf compresses have been used traditionally on various parts of the body that are sore and swollen
- cold should not be applied to nipples, especially if they are damaged, because it increases the chance of nipple vasospasm and consequent deep burning radiating breast pain. Ravaged nerve endings in traumatised nipples seem prone to triggering otherwise unprompted disturbances of blood flow to the nipples (vasospasm). It is a spontaneous constriction of blood vessels in the nipple. Blood vessels normally contract on exposure to cold, so cold applied to damaged nipples can be expected to cause additional vasospasm episodes.
- restricting the mother’s fluid intake will not usually have any impact on oversupply, but because of dehydration may increase the risks of blocked ducts, mastitis, breast infection and urinary tract infection for the mother
- rest helps a mother to conserve her physical resources and reduce the risk of breast infection. As much horizontal rest as possible helps the mother to fend off trouble. Typically, women who have been pushing themselves too hard, not ‘tuning in’ to their own needs, are more at risk of mastitis and breast infection. It is often a great surprise for first-time mothers to find that it takes far less activity than usual to make them feel quite drained. A stress diagram (Figure 6.3) is useful to help women reassess how they expend precious personal resources like time and energy
- engorged breasts may be soaked in warm (not hot!) Epsom salts solution until the temperature of the solution returns to tepid levels, taking care to wash it off the breasts before feeding or expressing milk for the baby. About a quarter to a half a cup of Epsom salts (Magnesium Sulphate) is dissolved in about two litres of warm water – ice-cream containers work quite well. The mother leans forward over the tubs, lowering her breasts into the solutions, resting her forearms on either side of the tubs for support while soaking her breasts. The resulting osmotic flow greatly reduces the tissue oedema that often accompanies acute oversupply. I don’t use this treatment now because I find vibration to be quicker, more effective and less messy
- antibiotics are not indicated unless the mother has symptoms of breast infection – a sore breast and ‘flu’ symptoms. Even then, only 20 percent actually have an infection and it is usually possible for her to ‘feed her way through’ early mastitis signs without antibiotics, as long as symptoms are not too severe – and the ongoing trend is obvious steady recovery
To do so, the mother needs to monitor her symptoms while following the recommended management regime previously discussed. She should be:
- no worse 2-3 hours after onset of the potential infection, preferably feeling better
- feeling much better 3-5 hours after symptoms began
- free of most or all of her symptoms 6-8 hours after onset
- completely free of symptoms 12-24 hours after onset
- some women with mastitis prefer to see their doctors anyway, ask for a prescription for antibiotics, buy them at the pharmacy and have them on hand should symptoms worsen
- if a mother is feeling really ill, or her symptoms are quickly worsening, she needs to see a doctor for antibiotic therapy immediately

‘Mastitis’ is a general term for an inflamed breast (left). Without ‘flu symptoms’, this is not a breast infection. Even then, only 20 percent of mothers with a sore breast and ‘flu symptoms’ actually have an infection, therefore resolving the inflammatory symptoms of mastitis must be the top priority for fast recovery. (133-134)
Basic management plan for mastitis
This mother does not have a breast infection (below left), because her only symptoms at this stage are a slightly sore, reddened breast. She does not need antibiotics. Even if she had ‘flu’ symptoms, she does not automatically need antibiotics as long as she manages her symptoms carefully.
It is not a situation to panic over, but simply to deal with as soon as she realises she has a problem:
- good breast drainage is paramount, from a well attached baby, or by expressing enough off to restore breast comfort
- taking an anti-inflammatory drug such as ibuprofen (Nurofen) or Voltarin (three times daily after meals) ‘takes the steam out’ of the inflammatory response. Paracetamol can be taken as well if needed for extra pain relief. (Paracetamol is not anti-inflammatory.)
- DO NOT APPLY HEAT! You would not be advised to put heat on any other inflamed part of your body!!
- use vibration on sore breasts (at least 10 minutes every hour)
- REST! Spend as much time lying down as possible to allow your body more resources for healing (135)
- as quickly as symptoms appeared, they can also be lost!
Seeing the doctor with symptoms of a breast infection
Sick mothers need to spend as little time away from home and bed as possible. Ringing ahead to find out if the doctor’s appointments are running to time, making it clear to reception staff that she is too unwell to sit while waiting can help to streamline the process. It is worth asking if they are able to put her into a room where she can lie down as soon as she arrives.
- Amoxicillin is contraindicated for breast infections because it is NOT EFFECTIVE against the likely infective organism, Staphylococcus aureus. Unfortunately, Amoxicillin – like all antibiotics – has some anti-inflammatory effect that relieves some of the impact of symptoms, so it can seem that the drug is effective. Instead, it commonly masks a worsening infection that may escalate into breast abscess. (157-166)
- Keflex (Cephalexin) may be effective against aureus, but is not generally as effective as Flucloxicillin or Dicloxicillin. However, the latter two drugs carry a potential risk of quite nasty side effects for some people, so I can understand some doctors’ anxieties about prescribing them. (166)
One of my local GPs explained that after two of his breast infection patients developed chronic liver damage in the same week after taking one of the latter two drugs, he will prescribe Keflex first in future in the hope that it will do the job. The downside of this approach is that it carries an increased risk of breast abscess if Keflex is not effective. Not an easy decision for doctors! Just another reason to tackle symptoms early so antibiotics are hardly ever needed!
A pituitary tumour (prolactinoma) can cause elevated prolactin levels, known as ‘hyperprolactinaemia’. Both men and women can develop the condition and lactate. If a woman with this condition is breastfeeding, she may have ongoing issues with uncontrollable oversupply (hyperlactation). Not surprisingly, there is not much information about prolactinomas and breastfeeding in medical literature, but the consensus is that these women can be encouraged to breastfeed as long as they are not taking anti-pituitary drugs while doing so. (These drugs could interfere with infant pituitary function.)
Generally, hyperprolactinaemia is not expected to worsen as a result of breastfeeding, but whether due to breastfeeding or not, I have had one case of this. During the six months she breastfed, ‘Pru’ had persisting episodes of engorgement that were at first resolved with a drink of sage tea once a month. But the incidents became increasingly frequent till she needed several sage teas every week by the time her baby was six months old. At this point her endocrinologist felt that Pru needed to wean and go back onto the drug she’d taken to control her condition before getting pregnant.
Other causes of hyperprolactinaemia in both men and women include damage to cervical nerves (such as from a car accident) and severe liver damage (such as cirrhosis of the liver).
Breast abscess was once a notifiable illness in Australia – around the 1940-50s. It coincided with an era when the prevailing medical advice for mastitis was ‘don’t feed, don’t express, and bind the breasts up firmly with a breast binder’! The pain must’ve been excruciating, and in the light of current knowledge, it is understandable that breast abscesses were quite common.
The worst possible timing for sudden weaning is when a mother has mastitis symptoms. Doing so increases the risk of infection because of a simultaneous sharp drop in antibodies in the milk. If infection is already present, abrupt weaning creates a far greater risk of abscess formation. Breast abscess is usually a preventable complication of poorly managed mastitis. The crux of prevention is good breast drainage, avoiding long periods of painful milk stasis and prompt, effective treatment of inflammatory breast symptoms (as previously explained). Breast abscess is also more likely after ineffective antibiotic therapy. (174)
An abscess is the body’s way of ‘sealing off’ an infected area to prevent surrounding tissues becoming infected. Perplexing to mothers with a breast abscess is that they may feel quite well, other than local soreness if the abscess is pressed on, although they may have had quite severe mastitis leading up to abscess formation. It shows the effectiveness of an abscess as local protection! The disadvantage is that neither antibiotics nor the body’s immunological defences can reach the contents of the abscess, so treatment after abscess encapsulation involves external penetration and drainage of its contents (pus and broken down body tissues).
Treatment options for breast abscess involve various combinations of: (174-177)
- fine needle aspiration
- indwelling catheter drainage
- surgical drainage (especially for large abscesses)
- antibiotics
Any surgical incisions are best made radially, considering the internal structures of the breast and preservation of breastfeeding after surgical drainage as well as for future lactations.


This sequence of pictures shows the crucial importance of good breast drainage to the health and comfort of breastfeeding women. On the left, a badly inflamed breast is shown before the baby’s first ever well attached breastfeed at 8 weeks of age. Then the breast can be seen already considerably less inflamed even during the feed, and finally the far more comfortable mother shows the wonderful contrast immediately after this breastfeed. As shown here, an optimally attached, effective baby is more useful for optimal breast drainage than trying to vary his feeding positions at the breast as is often suggested. Although it is still painful to feed from such a sore breast, it is important to do so as much as possible with a well-attached baby, in the interests of good breast drainage. The mother was in hospital on intravenous antibiotics for severe breast infection when these pictures were taken. Breast infections are largely preventable and should almost never progress to extremes like this. Prevailing advice to apply heat to already inflamed breasts is often involved in such cases.
‘Mastitis overkill’ is unfortunately very common:
The mother of a three week old baby, desperate for relief from mastitis symptoms, said that she just couldn’t keep up the almost non-stop effort midwives had advised was necessary to prevent her from developing a breast infection. She was almost frantic that she was going to have to wean because there was so much work involved that she was exhausted.
Presenting Scenario
- mastitis began 3 days earlier in left breast (red, sore, lumpy), but now mostly affecting right breast
- sore nipples
- baby delivered by emergency Caesarian. Mother still a bit stiff and sore abdominally. Needs physiotherapy for separated abdominal muscles ‘when she has the time’
- older child is 2½ years old, with a history of food allergy, eczema, colic, gastric reflux and can be described as hyperactive. He was breastfed for 6 months
- mother has allergy history of ‘normal childhood tonsillitis and ear infections’, and adult history of sinusitis
- husband is in a new job, very stressed about it, and away 3-5 days each week for work
- mother’s own mother fortunately lives close by and has been able to come and stay overnight every night so far
- even so, mother is exhausted from broken sleep – baby waking about every 1½-2 hours night and day
- baby has gained 430g in the last fortnight
- hospital midwives’ advice:
- rest as much as possible
- apply heat packs to both breasts
- massage the lumps out
- express off whatever she can when she is uncomfortably overfull if feeding does not relieve it
- mother unable to rest because she is constantly busy with breast massage, heat packs and expressing in between frequent feeds
- she is becoming increasingly upset because she is not making any headway against mastitis symptoms
90% Resolution within 5 hours by:
- discontinuing heat packs
- discontinuing breast massage in favour of intense vibration (at least 10 minutes every hour when mother is awake, until breasts are consistently lump-free)
- taking anti-inflammatories such as ibuprofen 3 times daily after meals
- the above three recommendations were enough to make further expressing unnecessary
- mother ecstatic that she can finally get some rest
Further resolution after:
- mother seen in Clinic 24 hours after initial phone conversation
- correcting sub-optimal attachment and positioning for breastfeeds – mother excited to have her first pain-free feeds!
- discontinuing mother’s flavoured, coloured Vitamin C tablets – take plain white ascorbate tablets instead – baby unlikely to tolerate additives in former tablets
- 6,000mg of fish oil daily for mother – NOT the odourless, processed one
- maternal dairy elimination rapidly reduced baby’s feeding frequency
- more peaceful baby, settling better after dairy exclusion. Baby also more satisfied with far better feeds
If breast lumps are no better beyond 24 hours from onset – usually after inappropriate or inadequate treatment – the first approach is 4 – 6 hours of 10 minutes of vibration hourly along with treatment measures already described to see if major progress can be made. If not, one or two ultrasound treatments are indicated as a preventative measure against breast infection and abscess. Physiotherapists are trained in the use of ultrasound therapy. Seeing a physiotherapist does not require a doctor’s referral.
The benefit of ultrasound is not necessarily obvious immediately after it is done, but its impact builds up over the following six to eight hours, during which vibration can also be used. A follow-up ultrasound treatment may be needed twelve to twenty-four hours after the first if there has not been enough resolution of the problem. (179-182)
There are two situations which automatically warrant ultrasound treatment:
- persisting unresolved blocked ducts especially those that persist beyond one or two days! This presumes that milk blebs are not responsible for the blockages
caked breast, a nasty situation with a breast that is just a solid mass of blocked ducts. Nothing can be expressed from a caked breast, and the baby can’t take anything from it either! It is, of course, very painful!
There is some controversy in the research about whether or not ultrasound treatment for mastitis is effective. (180-182)
Ultrasound (U/S) is very effective for resolving blocked ducts, as per the original article published in 1981. Where blocked ducts have been part of a clinical picture of breast infection verging on becoming an abscess, I have also known ultrasound to be very effective. (179)
However, U/S does not alleviate breast engorgement. (183)
There may be some changes in the doses of U/S used by some physiotherapists since the 1981 paper was published. A client also told me of her U/S breast treatment done through another material (like a solid gel) placed over her breast. It was not an effective treatment. Hence, the dose and other conditions of treatment may account for some failures in its effectiveness.
Warning – Some physiotherapists want to massage the breast after ultrasound treatment. I can’t recommend this! Physiotherapists are more used to massaging muscles, something which can be done fairly firmly, but breasts are not muscular in nature! I have had a number of cases where physiotherapist massage has caused bruising and more pain, which then has caused infection or made an already existing infection worse!
Finally…
We have an amazing preoccupation with undersupply that is far more likely to be imagined than real. Perceived undersupply can be responsible for maternal stress levels off the Richter Scale because of the imposed extra work of expressing and feeding deemed necessary for a milk supply to survive. A more realistic understanding that all this is usually unnecessary would result in more long term breastfeeding than is currently happening. Even when there is a need to increase milk production, it can usually be achieved more simply and easily than is indicated by prevailing advice.
There needs to be greater focus on understanding breastfeeding and assessing milk transfer, optimal attachment and positioning for breastfeeds – along with more emphasis on the story told by the contents of the baby’s nappy. Ideally, nappy output used as the clearest, simplest everyday indicator of infant milk intake should be part of general community knowledge, not needing to be formally taught to parents and health care providers as is the current situation.
Painful breast engorgement should be relieved long before it becomes extreme. Prompt attention to mothers’ breast comfort can make the difference between weaning and enjoyable breastfeeding experiences – or many days of painful, avoidable complications that become extremely expensive to families and our already overburdened health care system.
Better informed management of all supply issues means far greater breastfeeding satisfaction for mothers. What a great gift for women and babies, with millions of dollars’ worth of health benefits for the entire community!